“Won’t my cholesterol get worse and increase my risk of heart disease if I eat more fat?”
I get asked this question at least 3-4 times a day. The answer is, “NO. Not if you cut out the sugar and starch.”
“But, wait?! What about my heart? All that fat can’t be good for my heart?” they ask.
Cholesterol Defined
Let’s start with the contents of the standard cholesterol panel or “Lipid Panel.”
For the last 20-30 years the following labs have been looked at as the holy grail of heart disease risk:
- Total Cholesterol
- HDL (the measured number for “good” cholesterol)
- LDL-C (the calculated number for “bad” cholesterol).
- VLDL-C (the calculated number for very low density cholesterol)
- Triglycerides
The first problem with this panel is that it makes you believe that there are four different forms of cholesterol. NOT TRUE!
Actually, cholesterol is a steroid precursor that either makes up a part of the lipoprotein molecule or is transported with the triglycerides as a passenger. The lipoproteins are just transporters made of lipid that are only slightly different from their passenger load (causing increased or decreased density). The proteins that are contained within the wall of the lipoprotein transporter is what makes them different. These lipoprotein particles can be thought of, simplistically as buses, carrying triglyceride passengers. Here size does matter, and size determines the function of the molecule at that moment in time.
Cholesterol is Really Just a Triglyceride Bus
These buses, big and small, carry the passengers up and down the vascular system of the body. Glucose can float freely through the blood stream, but the other form of fuel, triglyceride, must be transported via the “lipoprotein bus”. The triglyceride and cholesterol are actually the passengers inside the bus. But triglyceride presence in the system seems to change the density of the lipoproteins. So now picture big, medium and small buses . . . the high density lipoprotein (HDL), intermediate density lipoprotein (IDL) and the low density lipoprotein (LDL) buses.

Triglyceride Changes the Density of Cholesterol
The density of the bus gets lower as triglyceride levels rise and fewer cholesterol esters and proteins are bound. As HDL goes up, LDL-C goes down (Parker TS et al, Proc Natl Acad Sci USA, Feb 1986)
The second problem is the VLDL-C and LDL-C are actually calculated numbers and don’t actually reflect the true presence of the lipoprotein particles as the triglyceride number rises. For the accountants, mathematicians and engineers reading this that calculation is called the Friedwald Equation and is as follows:
- LDL-C mmol/L = [Tot Cholesterol (mmol/L)] – [HDL-C (mmol/L)] – [TG (mmol/L) / 2.2]
- LDL-C mg/dL = [Tot Cholesterol (mg/dL)] – [HDL-C (mg/dL)] – [TG (mg/dL) / 5]
- VLDL-C = [TG / 5] as a calculated estimate
- This equation falls apart when the triglyceride level is greater than 400 mg/dL (4.52 mmol/L) or patients with hyperinsulinemia.
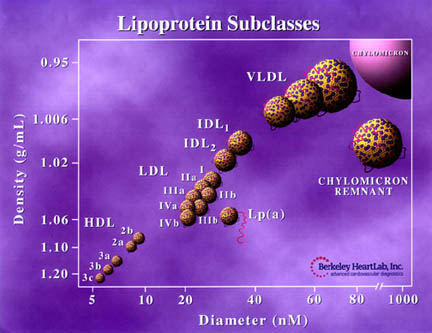
Total Cholesterol is the sum of the HDL, LDL, as well as intermediate density lipoprotein (IDL) & very low density lipoprotein (VLDL) which aren’t reported in the “Lipid Panel” above. So, total cholesterol is basically the sum of all the buses you have driving around.
The third key piece of information that the Lipid Panel above doesn’t tell you is the lipoprotein categories (HDL, LDL, IDL, and VLDL) are actually have three to four sub-types or sub-particles that are further differentiated by weight and size.
Improvement in cardiovascular risk, including improvement in cholesterol, inflammation and plaque formation have been the case with every patient I have used a high fat, low carbohydrate (ketogenic) dietary approach with over the last 12 years.
I’ve had so many people ask me how this works, and then, how to explain the changes to their primary doctors or cardiologist, I decided to write the following article. My intent is not to point the finger where others are wrong; but to identify how we, myself included, took a misstep along the path of scientific discovery. This misstep led to guidelines that, for over 45 years, have been accepted by medical students and clinicians as the “gospel truth.”
History of Cholesterol Measurement
The measurement of cholesterol, specifically total cholesterol, started in the 1950’s. There appeared to be a mild correlation of heart disease in countries who’s diets had higher fat intake. Ansel Key’s identified this apparent correlation in his Diet-Heart Hypothesis published in JAMA in 1957. He stated from his observational work that “the results of a fatty diet are hypercholesterolemia [elevated cholesterol].” A number of studies at the time showed that increasing fat intake in the standard diet increased total cholesterol; however, NO LINK to heart disease was ever proven (Ahrens EH, Jr, Lancet, May 1985).
Studies published by E. H. Ahrens, Jr. demonstrated that the cholesterol increased because of carbohydrate intake, not fat alone (Ahrens EH Jr, et al., Trans Assoc Am Physicians, 1961). The actual question, “Does increasing fat alone cause heart disease?” was never answered. The question, as well as known evidence based cholesterol reducing dietary approaches, were ignored in 1984 by the National Institutes of Health (NIH) Consensus Development Conference on Lowering Cholesterol to Prevent Heart Disease that was based heavily on epidemiological data rather than clinical reproducible science (Ahrens EH, Jr, Lancet May 1985).
Despite significant scientific evidence refuting the Diet-Heart Hypothesis, the 1984 NIH decision reflected politics and massive publicity campaigns.
Stop Demonizing My Eggs!
Since 1984, fat and cholesterol containing foods are treated like witches of Salem. As an example, eggs, specifically the egg yolk. (To this day, the chef at every breakfast bar I’ve ever visited asks if I want an egg white only omelet.) Interestingly, there is actually no scientific data association between whole egg consumption and heart disease. The science simply does not exist. Seriously, check for yourself.

You can’t extrapolate mortality risk based on a single small study that doesn’t actually identify correlation or causation. But the AHA did exactly that in 1961, and they are trying to do it again today. The MR-FIT study, largest study ever completed, is incessantly quoted as the study that demonstrates reduction in cholesterol leads to reduction in cardiovascular disease, but this trial was actually a failure and did not demonstrate improved risk by lowering cholesterol. In fact, the Director of the study, Dr. William Castelli actually stated, “. . . the more saturated fat one ate, the more cholesterol one ate, the more calories one ate, the lower people’s serum cholesterol…”
“We found that the people who ate the most cholesterol, ate the most saturated fat, ate the most calories weighed the least, and were the most physically active,” he said.
Diet-Heart Hypothesis Doesn’t Explain the French Paradox
To add to cholesterol confusion, the Diet-Heart Hypothesis does not explain the “European or French Paradox.” The French prefer cooking in butter instead of vegetable oil. In fact, the French eat 40% fat in their diet. And, more than 15% of that is saturated fat.

Interestingly, the French and those that eat the most cheese, butter and whole eggs have the lowest rate of coronary vessel calcification and heart disease. Attempts to explain this away as epidemiological error or diet complexities have been published, but still never answers the underlying question, “Does increasing fat alone cause heart disease?” (Ferrieres J, Heart, Jan 2004).
According to the Diet-Heart Hypothesis, people with familial hypercholesterolemia should have much shorter lifespans and are at increased risk of early mortality or death. However, there is actually no scientific evidence of this. In fact, the Honolulu Heart Program study revealed that people with low cholesterol are the ones at significant risk of early mortality or death (Schwartz I, et al., Lancet 2001 Aug). Additionally, higher LDL-C is actually predictive of longer life and has been demonstrated to correlate with longevity (Ravnskov U et al., BMJ Open, 2016 Jun 12;6(6): e010401).
Saturated Fat Isn’t Bad
I hate to burst your bubble, but saturated fat is NOT linked to vascular disease, diabetes or increased mortality (de Souza RJ et al., BMJ 2015,351:h3978).
It is commonly understood that LDL-C will rise as you eat more saturated fat. This is normal on a ketogenic diet. It has been reported in the scientific literature for over twenty years. It is to be expected, because LDL-C is really a measurement of three different LDL sub-particles (“big fluffy, medium, and small dense”). Increased saturated fat intake, while at the same time lowering carbohydrate intake, actually causes a shift in these low density particles to a bigger “fluffier” particle conformation (Griffin BA et al., Clin Sci (Lond), 1999 Sep). We know that the small dense LDL particles are the atherogenic / inflammatory particles participating in the formation of vascular disease and directly correlate with triglyceride levels. We also know the big “fluffy” LDL particles actually reduce the risk of vascular disease (Griffin BA et al., Clin Sci (Lond), 1999 Sep).

Why Do Physicians Still Prescribe STATIN Medications?
So why have clinicians been pushing the use of STATIN medications to reduce risk of coronary heart disease? It started with the Lipid Research Clinics Coronary Primary Prevention Trial (LRC-CPPT). This was a study of over 3800 men treated with cholestyramine, a cholesterol lowering medication (JAMA, 1984 Jan. 20;251(3):351-64.). There was a very slight “absolute reduction” in coronary heart disease risk, 1.6% to be exact. LDL-C decreased, but there was no reduction in the risk of death. In fact, there was actually an increase in risk of all cause mortality in the cholestyramine group which was never emphasized.
Overall, cholestyramine reduced non-fatal heart attacks in 60 of the 3,806 men. In other words, one in 63 men improved with the use of this medication . . . not very impressive. However, statistics look more impressive expressed in terms of “relative risk.” Relative risk is the percent increase of those with no treatment from those with treatment. This is always a bigger number.
When the LRC-CPPT researchers calculated relative risk, the percent change between the treated and non-treated was 19%. This bigger number was reported as the “risk reduction.” For those that don’t know the difference between actual risk and relative risk, 19% sounds very impressive! (JAMA. 1984 Jan 20;251(3):351-64.)
False Evidence Emphasized By Relative Risk
This relative risk reduction drove the STATIN era we are well aware of today. Lipitor (atorvastatin) reduces heart disease risk by only 1%. However, when you use the term “relative risk reduction,” it has more psychological effect. Relative risk of 36% sells more drugs.
Crestor (rosuvastatin) was show to have an absolute risk reduction in heart disease by 1.2%. When run through the relative risk reduction statistic it has a claim of 44% relative risk reduction.
These big numbers emphasized false evidences in many clinician’s minds that reducing LDL-C must be really effectively reducing heart disease.
Knowing that the LDL-C doesn’t really give you a clear idea of heart disease risk. It becomes essential to know which type of LDL lipoprotein particle is the atherogenic or heart disease causing particle. Research now points to the small-dense LDL particle as the atherogenic molecule (Hoogeveen RC et al., Arterioscler Thoromb Vasc Biol, 2014 May; Ivanova EA et al., Oxidative Med Cell Longevity, 2017 Apr). Studies have identified that elevated small-dense LDL cholesterol correlates much more closely with risk for inflammation, heart disease and vascular disease (Williams PT, et al. Atherosclerosis. 2014 April; 233(2): 713-720.)
A Better Marker for Heart Disease Risk?
Recent research demonstrates that small dense LDL cholesterol is a better marker for prediction of cardiovascular disease than total LDL-C (Hoogeveen RC et al., Arterioscler Thromb Vasc Biol. May 2014, 34(5): 1069-1077l; Ivanova EA et al., Oxidative Med Cell Longev. 2017).
The 2015 British Medical Journal, referenced above, analyzed the relevant 19 peer reviewed medical articles that included over 68,000 participants. This review showed that there is no association of high LDL-C with mortality (meaning that an elevated LDL-C does not lead to an increased risk of death from heart or vascular disease).
In stark opposition to the landmark evidences above, the American Heart Association’s Presidential Advisory published their position in the June 20, 2017 issue of Circulation. I am well aware of their position. They claim that saturated fat is the cause of increased LDL-C. Further, they extrapolate that elevated LDL-C is associated with increase in cardiovascular disease death. This boldfaced claim is based on one single small four-year (2009-2013) literature review completed by the World Health Organization. It looked at very small studies lasting only 3-5 weeks and comprised in total only 2353 participants. That’s not nearly long enough to see fully effective cholesterol changes. And, none of the studies had any focus on carbohydrate intake, insulin levels or LDL sub-particle measurement (Mensink RP, Geneva: WHO Library Cataloguing-in-Publication Data, 2016).
Clinical Evidence Is Pointing to Ketogenic Lifestyles as a Key
In my office, I see up to 10% regression in carotid stenosis (blockage in the carotid arteries) each year when following a ketogenic dietary lifestyle. Evidence points out that higher fat intake and lowering of carbohydrate intake has a regression effect on plaque and thickness of the arterial wall. (Shai I et al., Circulation, Mar 2010.) And, increased small dense LDL cholesterol correlates with thickening of the carotid arterial wall (Gentile M et al., Clinica Chimica Acta,Naples, Italy Division of Cardiology, Nov 2013, DOI: 10.1016 / j.cca.2013.08.010)
Based on the large body of evidence that sits before us today, the use of total cholesterol and LDL-C to determine vascular disease risk are obsolete and ineffective tools. That’s why we focus on insulin, triglycerides and small dense LDL particles.
Are you worried about your cholesterol?
Is a ketogenic lifestyle right for you?
These are great questions that I hope I can answer. Check out this month’s Kickstart program if you’re just getting started. Or, click here to work with me individually on your ketogenic lifestyle and cholesterol.